
Skin Parasite Symptom Checker
Select the symptoms you're experiencing to identify potential skin parasites. This tool is for informational purposes only and should not replace professional medical advice.
Symptoms
Imagine scratching an itch that isn’t just a reaction to dry skin, but the work of a tiny creature living right under your epidermis. From mites that burrow in secret to fly larvae that hatch beneath the surface, skin parasites are both creepy and oddly captivating. This guide uncovers the most fascinating facts about the parasites that live in or lay eggs on your skin, showing how they survive, what they look like, and how you can protect yourself.
Key Takeaways
- Skin parasites include mites, hookworm larvae, sand fleas, botfly larvae, and more, each with unique life cycles.
- Most infections start when parasites enter through tiny cuts, barefoot walks, or direct skin contact.
- Symptoms range from intense itching to painful nodules; early detection prevents complications.
- Treatment often involves prescription topical or oral medications, but prevention is the best cure.
- Understanding parasite behavior helps you spot infections sooner and avoid long‑term skin damage.
What Are Cutaneous Parasites?
Cutaneous parasites are organisms that either live on the surface of the skin or embed themselves within the upper layers. They belong to diverse groups-arthropods, nematodes, and protozoa-yet share a common goal: using human skin as a host for feeding or reproduction. While many people think of parasites as something you find in the gut, skin‑dwelling species are just as widespread and often go unnoticed until they cause irritation.
Scabies: The Burrowing Mite
Scabies mite is a microscopic arthropod (Sarcoptes scabiei) that tunnels into the upper skin layer to lay eggs. A single female can lay up to 30 eggs over two weeks, and the intense itching comes from an allergic reaction to the mites, their feces, and the eggs. Scabies spreads through prolonged skin‑to‑skin contact, which is why it’s common in families and crowded living conditions.
- Typical sign: a rash of tiny bumps, especially between fingers, wrists, and the waistline.
- Key fact: The mite can survive off a host for up to 72 hours, so bedding and clothing can spread the infection.
Hookworm Skin Migration (Cutaneous Larva Migrans)
Hookworm larvae (Ancylostoma braziliense or Ancylostoma caninum) are tiny roundworms that penetrate the skin when you walk barefoot on contaminated soil. They cannot complete their life cycle in humans, so they wander through the epidermis, leaving a winding, itchy track known as "creeping eruption."
- Typical sign: a red, serpentine line that moves a few millimeters each day.
- Key fact: The larvae can survive up to two weeks in the skin before dying if they don’t reach a suitable host.
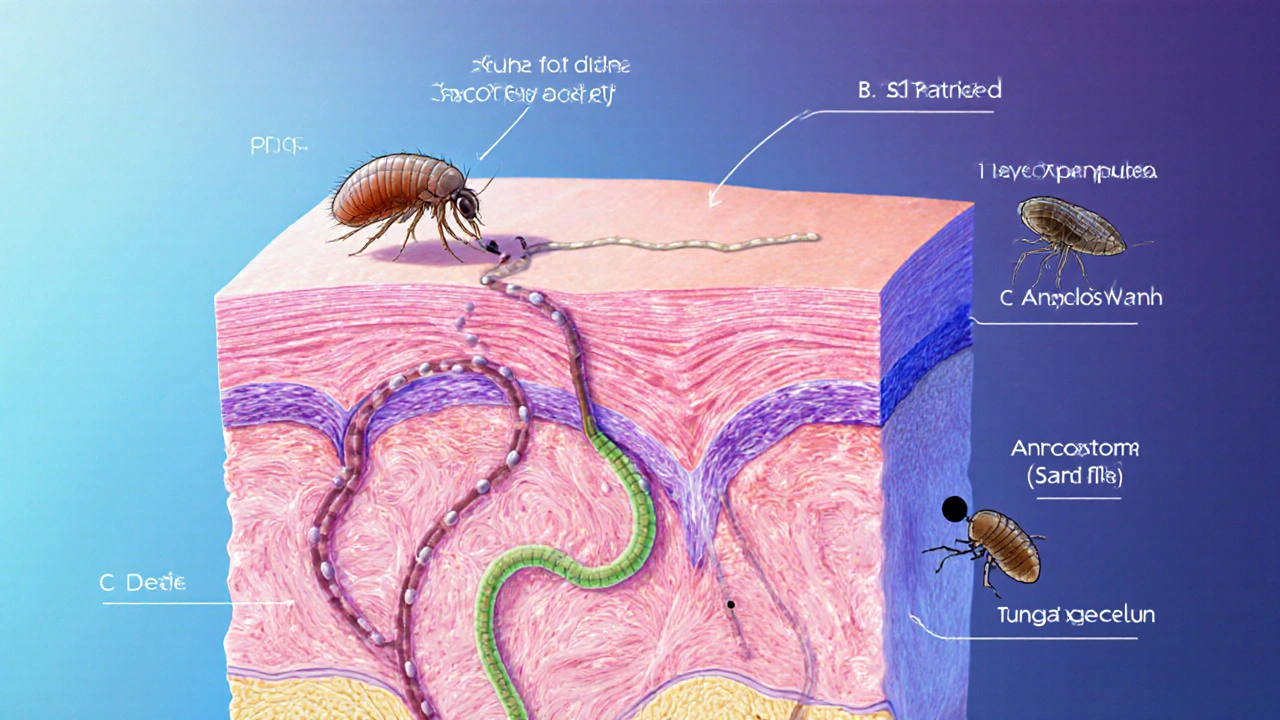
Tungiasis: The Sand Flea
Tungiasis is an infection caused by the female sand flea (Tunga penetrans) that burrows into the skin, usually on the feet. The flea embeds its abdomen into the epidermis, expands, and releases eggs onto the ground, completing its cycle within weeks.
- Typical sign: a painful, inflamed nodule with a small central black spot where the flea’s rear end protrudes.
- Key fact: In heavy infestations, multiple fleas can cause secondary bacterial infections and even lead to tetanus if untreated.
Botfly Larvae: The Hidden Grub (Myiasis)
Botfly larvae (Dermatobia hominis) are fly larvae that enter the skin when a mosquito or other carrier deposits their eggs on a host. Once inside, they develop into a painful, boil‑like lump that eventually erupts, allowing the mature larva to exit.
- Typical sign: a raised, tender nodule with a central opening that occasionally breathes.
- Key fact: The larva can stay inside for up to 12 weeks, growing up to 2 cm before emerging.
Cheyletiella: Walking Dandruff
Cheyletiella is a genus of tiny mites (often called "walking dandruff") that live on the skin of animals and occasionally humans. The mites are visible as moving specks of white or gray on the skin surface, causing intense itching.
- Typical sign: fine, moving scales that can be seen with the naked eye or a magnifying glass.
- Key fact: Transmission usually occurs through close contact with infected pets, especially cats and dogs.
Demodex: The Invisible Resident
Demodex folliculorum is a microscopic mite that lives in hair follicles and sebaceous glands of the face and scalp. Most people host a few dozen without any symptoms, but overgrowth can trigger rosacea‑like redness and itching.
- Typical sign: persistent facial redness, itching, or a sensation of “ticks” in the skin.
- Key fact: Studies show a higher Demodex density in individuals with compromised immune systems.

Cutaneous Leishmaniasis: The Sandfly Parasite
Cutaneous leishmaniasis is a skin infection caused by protozoan parasites of the genus Leishmania, transmitted by the bite of infected sandflies. It creates ulcerated sores that can persist for months if untreated.
- Typical sign: a painless papule that later ulcerates, often on exposed areas like the arms or face.
- Key fact: Over 1 million new cases are reported worldwide each year, with the disease prevalent in tropical and subtropical regions.
How to Spot and Treat Skin Parasite Infections
Early recognition is crucial. Look for persistent itching, unusual rashes, moving specks, or nodules that don’t heal.
- Consult a dermatologist or primary care provider. They can perform skin scrapings, needle aspirates, or biopsies to identify the parasite.
- Follow prescribed medication. Topical permethrin works for scabies, while oral ivermectin can treat many mite and larval infections.
- Maintain hygiene. Wash affected areas with gentle soap, keep nails trimmed, and avoid scratching to prevent secondary bacterial infection.
- Treat the environment. Wash bedding, clothes, and shoes at high temperatures to kill off any lingering stages.
Prevention Tips
- Wear shoes outdoors in tropical or sandy environments to block hookworm and sand flea larvae.
- Avoid direct skin contact with infested animals; use gloves when handling pets that show excessive itching.
- Apply insect repellent containing DEET or picaridin on exposed skin when traveling to sandfly‑prone regions.
- Regularly clean and vacuum carpets and bedding to reduce mite reservoirs.
- Seek prompt medical care for any suspicious skin lesions, especially after travel.
Comparison of Common Skin Parasites
| Parasite | Scientific Name | Transmission | Typical Symptoms | Treatment |
|---|---|---|---|---|
| Scabies | Sarcoptes scabiei | Prolonged skin‑to‑skin contact | Intense itching, burrow tracks | Permethrin 5% cream |
| Hookworm larvae | Ancylostoma braziliense / caninum | Walking barefoot on contaminated soil | Serpentine, migrating rash | Ivermectin or albendazole |
| Tungiasis | Tunga penetrans | Contact with sandy ground with flea eggs | Painful nodules, central black spot | Extraction of flea, topical antibiotics |
| Botfly (Myiasis) | Dermatobia hominis | Eggs deposited by mosquito or other carrier | Boil‑like nodule, breathing opening | Surgical removal, antibiotics if infected |
| Cheyletiella | Cheyletiella yasuni (common species) | Direct contact with infested pets | Moving dandruff, itching | Sulfur shampoos, ivermectin |
| Demodex overgrowth | Demodex folliculorum | Normal skin flora, proliferates in immune‑compromise | Rosacea‑like redness, itching | Tea tree oil, metronidazole |
| Cutaneous leishmaniasis | Leishmania spp. | Sandfly bite | Papule → ulcerating sore | Miltefosine or antimonial drugs |
Frequently Asked Questions
Can skin parasites be transmitted from person to person?
Some, like scabies, spread through prolonged skin‑to‑skin contact. Others, such as hookworm larvae, need environmental exposure (soil) rather than direct person‑to‑person transfer.
Is it safe to treat skin parasites at home?
Mild cases like Demodex overgrowth can be managed with over‑the‑counter tea tree oil or gentle shampoos, but most infections require prescription medication and professional removal to avoid complications.
How long do these parasites survive on the skin?
Survival varies: scabies mites can live up to 72 hours off‑host; hookworm larvae survive a couple of weeks; botfly larvae stay embedded for months; Demodex mites can live for years as part of the skin flora.
Do skin parasites cause long‑term damage?
If untreated, secondary bacterial infections, scarring, or chronic inflammation can develop, especially with tungiasis or myiasis. Early treatment usually prevents lasting harm.
Can pets carry the same parasites that affect humans?
Pets are common carriers of Cheyletiella and can harbor Demodex species specific to animals. While they rarely transmit scabies to humans, they can pass fleas and mites that cause skin irritation.



Kyle Olsen
In the grand tapestry of dermatological pathology, the article presents a most pedestrian overview of cutaneous parasites, bordering on the banal. The author appears eager to enumerate species without delving into the nuanced immunological interactions that truly define host‑parasite dynamics. One might lament the omission of recent genomic insights that have revolutionized our understanding of Sarcoptes scabiei resistance patterns. Moreover, the discussion of treatment modalities neglects the emerging concerns about ivermectin resistance in certain endemic regions. The narrative, while thorough in breadth, lacks the depth that a discerning scholar would demand. Let us not forget the epidemiological shifts driven by climate change, which the piece fails to address. The lifecycle diagrams would benefit from a more rigorous temporal scaling, highlighting the latency periods that dictate clinical presentation. It is also noteworthy that the article glosses over the socioeconomic determinants that predispose vulnerable populations to infestations. Whilst the preventive measures listed are sound, they are offered without the contextual framing of public health infrastructure limitations. The tone oscillates between layman‑friendly and unnecessarily verbose, a duality that betrays uncertainty about the intended audience. In sum, the exposition serves as a modest primer, yet it does not ascend to the scholarly treatise it aspires to be. One hopes future revisions will incorporate these critical perspectives, thereby elevating the discourse from mere cataloguing to a truly enlightening exposition.
Sarah Kherbouche
Honestly this piece is a pathetic attempt to sound sci‑fi, and the US is always the one wimpin’ around for these creeps. They should’ve mentioned how the gov’t hides the real data about hookworm spread, lol. The whole "wear shoes" advice is just lazy filler, we needs real solutions, not that weak‑ass info. F*** that generic advice, get real!
MANAS MISHRA
I totally get where Kyle is coming from – the article could indeed dive deeper into the host immune response. Still, the inclusion of a simple symptom checker is useful for people who might not recognize early signs. It’s good that they highlighted both treatment and prevention. Keep up the balanced effort!
Lawrence Bergfeld
Well, you’ve got your facts and you’ve got your fluff; the article skims the surface, yet it does give a helpful quick‑check list; for those who need concise info, it serves a purpose; however, a deeper dive would be preferable.
Chelsea Kerr
Very informative! 😃 I especially appreciate the clear layout of each parasite’s life cycle – makes it easier to remember. 🌿🌎 The emoji‑style headings add a friendly touch, while the detailed treatment options are spot‑on. Keep the emojis coming! 😉
Tom Becker
They’re hiding the truth about the botfly, man. Got supspicious that the pharma industry wants us to think it’s just a “boil” so we keep buying their meds. Wake up, folks!
Laura Sanders
The article reads like a textbook written for undergrads. It lacks the sophisticated analysis expected from a seasoned scholar. Nonetheless, the table summarising parasites is a nice touch.
Jai Patel
What a vibrant dive into the world of skin squirmers! 🌈 From the sneaky sand flea to the mischievous botfly, each description bursts with color and life. The cultural tidbits about barefoot habits really hit home – reminds me of summer nights in Goa. Keep the energy flowing, this guide is a real eye‑opener.
Zara @WSLab
Great rundown! 😊 The step‑by‑step symptom checker makes it simple for anyone to get a quick idea of what might be happening. Your friendly tone encourages readers to seek professional help without fear. Keep up the supportive vibe! 👍
Randy Pierson
Your vivid descriptions paint a picture of each parasite’s sinister parade across our skin. I especially enjoyed the playful metaphor of “walking dandruff” – it’s both accurate and delightfully phrased. The balance between science and storytelling is spot‑on.
Bruce T
While the facts are solid, we must remember our responsibility to educate responsibly. Spreading awareness about these parasites is a moral duty; ignorance only fuels suffering. Let’s champion informed vigilance.
Darla Sudheer
Nice summary – concise and clear. Good job.
Elizabeth González
The exposition exhibits a commendable thoroughness, yet it would benefit from a more measured consideration of the socioeconomic contexts that predispose individuals to such infestations. A nuanced approach would elevate the discourse.
chioma uche
Our nation should stand proud in combating these parasites, ensuring no foreign invasion of skin goes unchecked. United we fight, united we heal.
Satyabhan Singh
The meticulous detailing of each organism’s life cycle reflects a profound respect for scientific rigor, befitting the scholarly tradition of our esteemed institutions. Such erudition is indeed laudable.
Keith Laser
Oh sure, another “how‑to” guide – because we all needed a 10‑minute lecture on itching. Sarcasm aside, the quick‑check tool is actually pretty handy for the clueless crowd.
Winnie Chan
Nice work, but let’s be real – most people will just scratch and hope for the best. Still, a friendly reminder never hurts.
Kyle Rensmeyer
Ever wonder why they don’t mention the hidden labs that study these parasites? There’s definitely more going on behind the scenes… 🤔
Rod Maine
One must consider the aesthetic presentation; the article’s layout lacks the sophistication expected of a premier scientific discourse.
Othilie Kaestner
Well, the guide does a decent job listing symptoms, but it could’ve dived deeper into preventive cultural practices. Still, a solid starting point for anyone curious.