Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis aren’t just rare skin conditions-they’re life-threatening drug reactions that can turn a simple prescription into a medical emergency. If you’ve ever taken an anticonvulsant, antibiotic, or gout medication, you need to understand the warning signs. These aren’t typical rashes. They’re full-body betrayals of your own immune system, triggered by medications you might never suspect are dangerous.
What Exactly Are SJS and TEN?
Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) exist on the same spectrum, but they’re not the same. Think of them as degrees of the same catastrophic reaction. SJS affects less than 10% of your skin surface. TEN? That’s more than 30%. In between? That’s called overlap, and it’s still serious. The difference isn’t just numbers-it’s survival. TEN has a death rate of about 25%. SJS? Around 10%. Both are medical emergencies that require hospitalization, often in burn units.
They’re named after the doctors who first described them. Stevens and Johnson in 1922 noticed two boys with fever, blisters, and peeling skin. Decades later, Dr. Alan Lyell documented the extreme form-where skin sloughs off like a burn. Today, we know it’s not about the name. It’s about how much of your skin is dying.
How Do These Reactions Start?
Most cases-over 80%-are caused by medications. It’s not random. Certain drugs carry known risks. Carbamazepine (for seizures), allopurinol (for gout), sulfonamide antibiotics (like Bactrim), and lamotrigine (for epilepsy and bipolar) are the usual suspects. NSAIDs, nevirapine (for HIV), and even some painkillers can trigger it.
But here’s the twist: it’s not just the drug. It’s your genes. If you carry the HLA-B*15:02 gene variant, taking carbamazepine raises your risk of SJS/TEN by 1,000 times. That’s not a small chance-it’s a red flag. In Southeast Asia, where this gene is common, doctors test for it before prescribing. The same goes for HLA-B*58:01 and allopurinol. In 2022, the FDA approved a point-of-care test that gives results in four hours. No more waiting two weeks.
Less common? Infections. Mycoplasma pneumoniae, the bug behind walking pneumonia, can trigger SJS in kids. But drugs are still the main cause.
What Does It Feel Like?
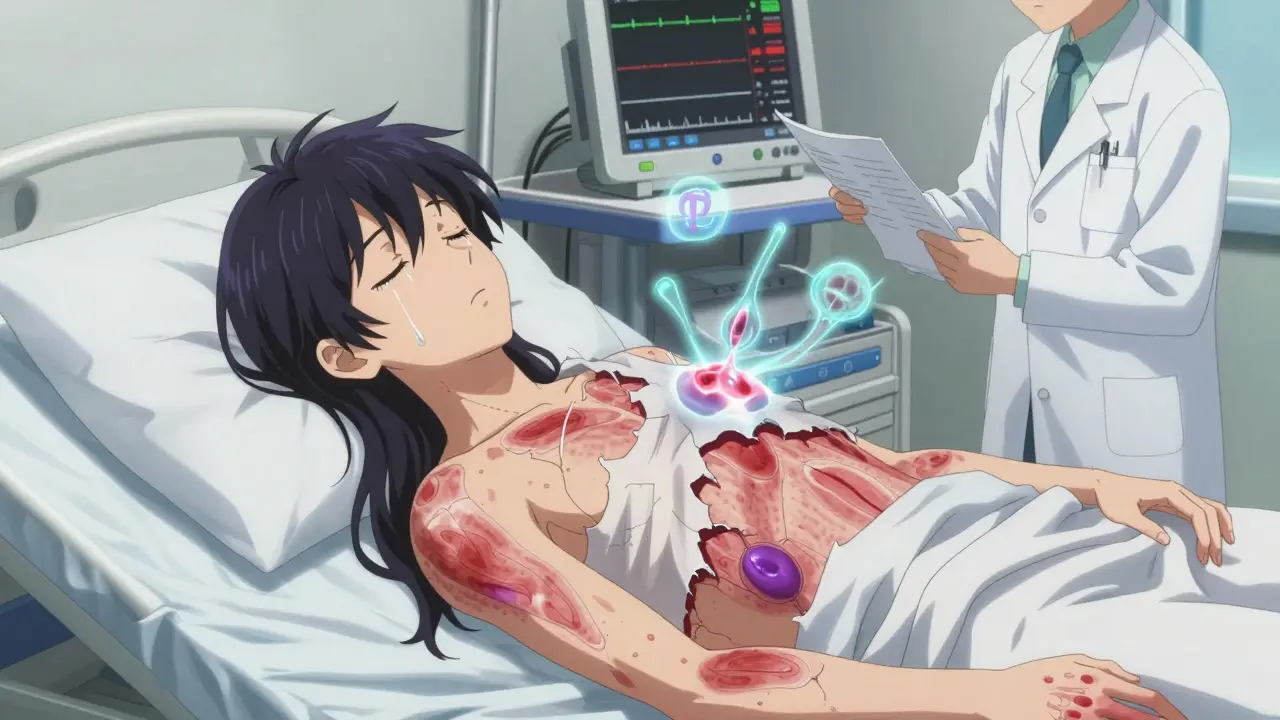
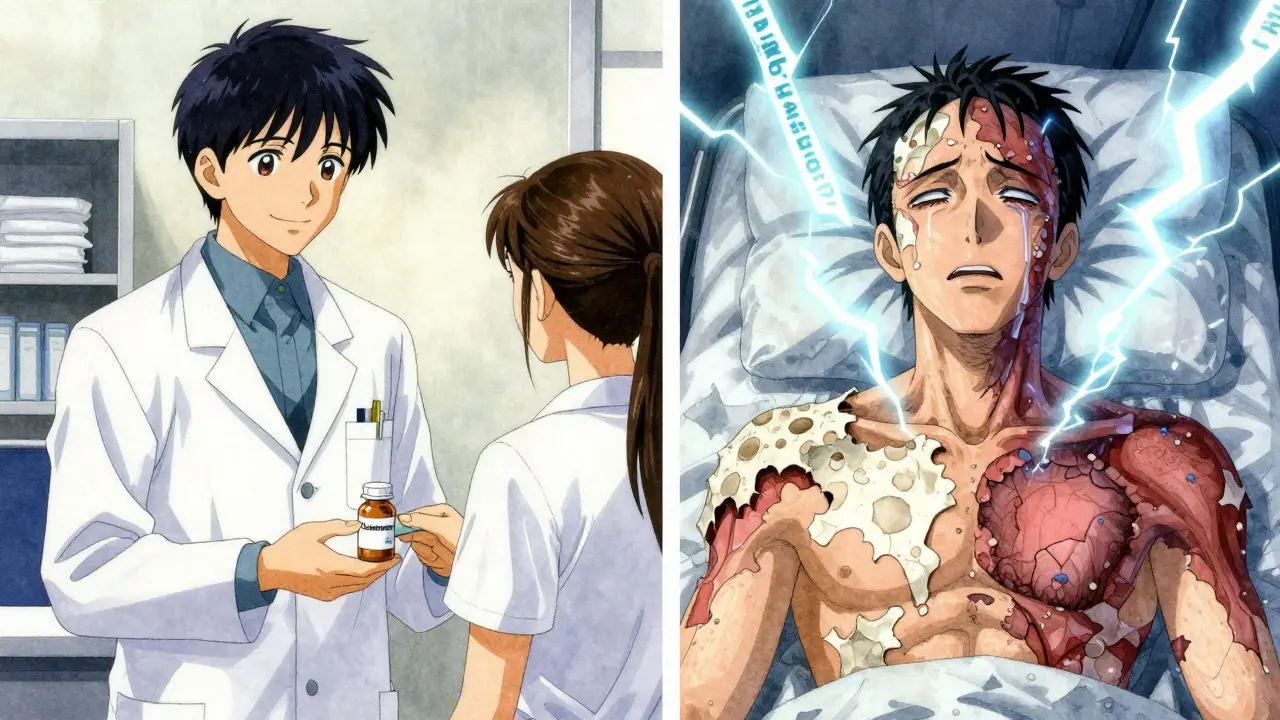
It doesn’t start with a rash. It starts with a fever-often above 102°F-and a sore throat, cough, or burning eyes. You feel like you’ve got the flu. Then, within a few days, your skin changes. Red or purple patches appear, usually on your chest or back. They spread fast. Within 24 to 72 hours, they turn into blisters. The skin starts to peel off in sheets. You can’t even touch your own body without pain.
And the mucous membranes? They’re destroyed. Over 90% of patients have mouth ulcers so bad they can’t eat or drink. Eighty percent have eye damage-burning, swelling, pus. Sixty percent get genital sores. Your skin isn’t just peeling-it’s dissolving. The Nikolsky sign? That’s when you gently rub the skin and it sloughs off. It’s a terrifying test doctors use to confirm it.
This isn’t a rash. It’s a full-thickness skin death. Your epidermis detaches from the dermis. It’s not infection. It’s your immune system attacking your own skin cells with a chemical called granulysin. It’s like your body turns on itself.
How Is It Diagnosed?
Doctors don’t guess. They confirm. A skin biopsy is the gold standard. Under the microscope, they see full-thickness epidermal necrosis-dead skin cells with almost no inflammation underneath. That’s what sets it apart from staph infections or other blistering diseases.
They also use the RegiSCAR criteria: sudden onset, skin tenderness, mucosal damage, and the right lesion pattern. Blood tests show high inflammation markers. But the real clue? Your medication history. Did you start a new drug 1 to 3 weeks ago? That’s your smoking gun.
What Happens in the Hospital?
First thing? Stop every non-essential drug. No exceptions. Even aspirin or a vitamin you’ve taken for years? Out. The culprit might be obvious, but you can’t afford to miss one.
You’ll be moved to a burn unit or ICU. Your skin loss is like a third-degree burn. You lose fluids, proteins, electrolytes. You need 3 to 4 times the normal IV fluids. You’re hooked to monitors for heart rate, blood pressure, kidney function.
Wound care is delicate. No adhesive bandages. Just soft, non-stick dressings. Pain control? That’s critical. You’re not just in pain-you’re in agony. Morphine isn’t optional.
Eye care? Daily visits from an ophthalmologist. Without it, you risk scarring, dry eyes, or even blindness. Half of survivors need lifelong eye drops.
Can It Be Treated?
There’s no magic bullet. And some treatments are controversial.
IVIG (intravenous immunoglobulin) was once thought to help. But large studies showed no real survival benefit. Steroids? They suppress the immune system, but they also increase infection risk-deadly when your skin is gone. Some doctors still use high-dose methylprednisolone early on.
Cyclosporine? A 2016 trial showed it cut mortality from 33% to 12.5%. It blocks the immune cells that kill skin cells. It’s now used in many centers.
Etanercept? A TNF-alpha inhibitor. A 2019 study gave it to 12 TEN patients within 48 hours. Zero deaths. Historical controls had a 31% death rate. That’s promising. It’s not FDA-approved for this, but it’s being used off-label.
What works best? Time, supportive care, and stopping the drug. The sooner you get into a specialized unit, the better your odds.
What Happens After You Survive?
Survival doesn’t mean recovery. Sixty to eighty percent of survivors have long-term problems.
Your skin? It might heal, but you’ll have dark or light patches. Scars. Nails that grow crooked. Your eyes? Dryness, light sensitivity, vision loss. Fifty percent need ongoing ophthalmology care. Your genitals? Urethral strictures or vaginal adhesions. Some need surgery.
And then there’s the mental toll. Forty percent develop PTSD. The pain, the isolation, the fear of dying-some never fully recover from that.
Can It Be Prevented?
Yes. And it’s already happening.
Taiwan started mandatory HLA-B*15:02 testing before giving carbamazepine. Between 2007 and 2013, SJS/TEN cases dropped by 80%. That’s not luck-it’s prevention.
The FDA now recommends genetic screening for:
- HLA-B*15:02 before carbamazepine in people of Asian descent
- HLA-B*58:01 before allopurinol in all ethnic groups
That’s why your pharmacist might ask about your ancestry. It’s not profiling-it’s saving lives.
If you’re prescribed one of these drugs and you’re not tested, ask why. Your doctor might not know. Or they might think it’s not needed. But the data is clear: genetic screening prevents death.
What Should You Do?
If you’re on carbamazepine, lamotrigine, allopurinol, or sulfonamides:
- Know your family history. Has anyone had a severe skin reaction?
- Ask your doctor about HLA testing before starting.
- Watch for fever, sore throat, or eye pain in the first few weeks.
- If your skin starts peeling or blisters appear-go to the ER. Don’t wait.
This isn’t a "maybe." It’s a "when." The window between a flu-like illness and full-body skin loss is as short as 48 hours. Speed saves lives.
Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis are rare. But they’re not random. They’re predictable. And now, with genetic testing and better awareness, they’re preventable.
Can Stevens-Johnson Syndrome be caused by infections, not just drugs?
Yes, though it’s less common. About 10% of pediatric cases are triggered by infections, especially Mycoplasma pneumoniae. In adults, over 80% are drug-related. But if you’ve recently had pneumonia or a severe flu and then developed blisters or peeling skin, it’s still possible. Always tell your doctor about recent infections.
Is SJS/TEN contagious?
No. It’s not an infection. It’s a severe immune reaction to a drug or, rarely, an infection. You can’t catch it from someone else. But if you’ve had SJS/TEN from a certain medication, you must never take it again-even a tiny amount can trigger a deadly recurrence.
How long does recovery take after SJS/TEN?
Skin healing takes 2 to 4 weeks, but recovery doesn’t end there. Mucosal damage, especially in the eyes and genitals, can take months to stabilize. Many survivors deal with chronic dry eyes, scarring, or pain for years. Psychological recovery can take even longer-some people need years of therapy to cope with the trauma.
Why do some people get SJS/TEN and others don’t, even with the same drug?
Genetics. Certain gene variants-like HLA-B*15:02 or HLA-B*58:01-make your immune system overreact to specific drugs. Without those genes, the risk is extremely low. That’s why testing before prescribing high-risk medications saves lives. It’s not about the drug alone-it’s about your body’s unique response to it.
Are there new treatments on the horizon?
Yes. Researchers are testing drugs that block granulysin, the protein that kills skin cells in SJS/TEN. Phase II trials are expected to begin in 2024. Other promising approaches include targeted biologics like etanercept, which has shown zero mortality in early studies when given within 48 hours. The future is moving from broad immune suppression to precise, targeted therapy.




Paul Ratliff
just got prescribed carbamazepine last week. read this and immediately texted my doc to ask about the gene test. they were like ‘oh yeah we do that now’ - turns out they’ve been doing it since 2021. wild how fast this stuff catches on if you ask.
SNEHA GUPTA
The mechanistic elegance of granulysin-mediated cytotoxicity in SJS/TEN is both terrifying and fascinating. It is not merely an immune overreaction-it is a targeted molecular betrayal. The fact that HLA alleles dictate susceptibility speaks to the precision of human immunogenetics. We are not merely patients; we are genetic signatures waiting to be read.
Gaurav Kumar
India has the highest genetic prevalence of HLA-B*15:02. Yet we still let doctors prescribe carbamazepine like it’s aspirin. Why? Because ‘we don’t have infrastructure’? Bullshit. We have more labs than the entire EU. This isn’t a medical problem-it’s a colonial mindset. Test everyone. Stop the bleeding. Stop the excuses.
David Robinson
Okay but let’s be real-how many people even know what HLA stands for? I’m a nurse and I had to look it up. The whole ‘genetic screening’ thing sounds cool, but most patients are gonna get confused and say ‘just give me the pill’. And doctors? They’re overworked. They’ll skip the test because ‘it’s not urgent’. This article is great, but it’s preaching to the choir. We need billboards. We need TV ads. We need a viral TikTok trend.
Jeremy Van Veelen
Imagine your skin-your literal barrier against the world-turning into ash because some chemist in a lab 20 years ago made a molecule that your body decided was a demon. That’s not medicine. That’s a cosmic joke. And now we’re supposed to be grateful because they have a four-hour test? That’s not progress. That’s damage control. We’re still playing whack-a-mole with our own biology.
Laura Gabel
my cousin had this after taking allopurinol. they put her in a burn unit. she lost 40% of her skin. now she can’t cry without her eyes burning. no one told her to get tested. no one even mentioned genes. this isn’t rare. it’s ignored.
jerome Reverdy
From a clinical immunology standpoint, this is one of the most elegant examples of pharmacogenomics in action. Granulysin as the effector molecule, HLA as the gatekeeper, and drug metabolism as the trigger-it’s a perfect storm of molecular recognition failure. The fact that we can now intervene preemptively with point-of-care testing is revolutionary. We’re moving from reactive medicine to predictive medicine. This isn’t just about SJS/TEN-it’s the blueprint for the future of personalized therapeutics.
Andrew Mamone
Just had a 3am panic scroll after reading this. 😱 My dad’s on allopurinol. I’m calling his doctor tomorrow. Also-etanercept? Zero deaths in 12 patients? That’s not a miracle. That’s a wake-up call. We need this everywhere. 🙏
Srividhya Srinivasan
THIS IS A BIG PHARMA SCAM. They don’t want you to know that HLA testing costs $120… but the drug? $3,000/month. They’d rather you lose skin than save money. And the ‘FDA approved test’? That’s just to make you feel safe while they keep selling you poison. Wake up. The real cure? Stop taking ALL synthetic drugs. Go organic. Drink lemon water. Your body knows better.
Stephen Habegger
Thanks for writing this. I’m a survivor. Took 3 years to get my vision back. Still need eye drops. But I’m alive. And now I tell everyone I know: ask before you take it. Seriously. Just ask.
Paul Ratliff
^^ this. i’m scared but also kinda hopeful. if we can prevent this with a quick test, why aren’t we doing it everywhere? it’s not rocket science.
Justin Archuletta
my mom’s on lamotrigine. i just texted her this article. she said ‘oh i thought that was just for epilepsy’… she’s 68. this needs to be on every prescription bottle.